Item addedItem updatedItem removedNo more products on stockYou entered wrong value.
No products in the cart.
Clinical Knowledge Centre
The Pegasus Clinical Knowledge Centre will provide a one-stop resource for patients, nursing staff and caregivers alike for useful information about pressure ulcers, guidance on pressure ulcer grading as well understanding the theories behind pressure care mattress systems.
Pressure Ulcers & Classification
Pressure ulcers, also known as decubitus ulcers, pressure injuries or bedsores represent a formidable health challenge worldwide, with significant financial implications for healthcare providers, increased workloads for nursing staff and a reduced quality of life for large numbers of patients.
The International NPUAP-EPUAP pressure ulcer definition is as follows:
A pressure ulcer is defined as a localised injury to the skin and/or underlying tissue usually over a bony prominence, as a result of pressure, or pressure in combination with shear and friction.
There are a number grading systems used by healthcare professionals to describe the severity of pressure ulcers. The most common is the NPUAP-EPUAP grading system, which is outlined below.
The unique features of Airwave Therapy are:
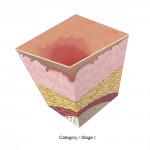
Intact skin with non-blanchable redness of a localized area usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area. The area may be painful, firm, soft, warmer or cooler as compared to adjacent tissue.Category I may be difficult to detect in individuals with dark skin tones. May indicate “at risk” persons.
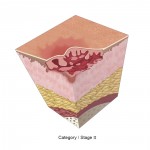
Category/Stage II: Partial thickness
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ruptured serum-filled or sero-sanginous filled blister. Presents as a shiny or dry shallow ulcer without slough or bruising*. This category should not be used to describe skin tears, tape burns, incontinence associated dermatitis, maceration or excoriation.
*Bruising indicates deep tissue injury.
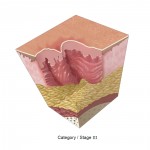
Category/Stage III: Full thickness skin loss
Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle are not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining and tunnelling.
The depth of a Category/Stage III pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and Category/Stage III ulcers can be shallow. In contrast, areas of significant adiposity can develop extremely deep Category/Stage III pressure ulcers. Bone/tendon is not visible or directly palpable.
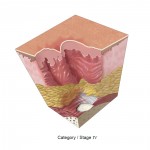
Category/Stage IV: Full thickness tissue loss
Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present. Often includes undermining and tunnelling. The depth of a Category/Stage IV pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput and malleolus do not have subcutaneous tissue and these ulcers can be shallow. Category/Stage IV ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon or joint capsule) making osteomyelitis or osteitis likely to occur. Exposed bone/muscle is visible or directly palpable
Source: Pressure Ulcer Prevention and Treatment EPUAP Review Guideline written by the European Pressure Ulcer Advisory Panel (2009).
Causes of Pressure Ulcers
Pressure ulcers are the result of sustained external forces being placed on a particular part of the body.
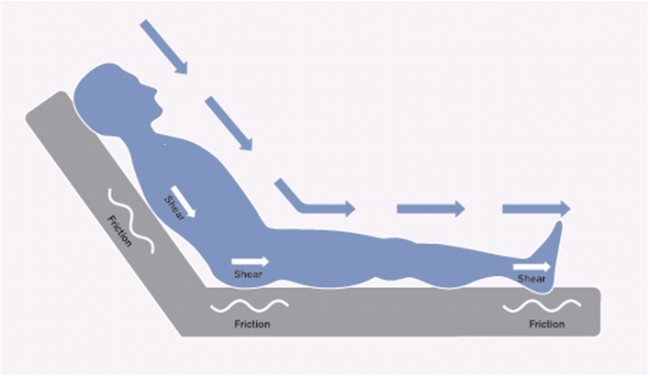
The application of external forces such as pressure, shear and friction interrupt the blood supply to the affected area of skin meaning that vital elements that keep tissues healthy such as oxygen and nutrients are restricted and without a constant blood supply, tissue is damaged and will eventually die and a pressure ulcer form.
Pressure:
Applied local or point pressure compresses and distorts the body tissue between the support surface and a persons bony prominences causing the occlusion of capillary blood flow resulting in tissue damage.
Shear:
Applied local or point pressure compresses and distorts the body tissue between the support surface and a persons bony prominences causing the occlusion of capillary blood flow resulting in tissue damage.
Friction:
Friction is the resistance to motion of the external tissue sliding in a direction parallel to the support surface. Friction may contribute separately to pressure ulcers by stripping superficial skin layers and causing ulceration. The heels are especially at risk particularly when a person is being repositioned up the bed. Usually occurs at anatomical sites subjected to frequent friction e.g. the heels or sacrum. Causes external skin damage, such as blistering or breaks.
Moisture:
Incontinence of urine and faeces can contribute to pressure ulcer formation around the buttocks, sacrum and hip regions. The moisture can lead to maceration and the urine and faeces act as skin irritants that promote skin breakdown.
Common Locations of Pressure Ulcers
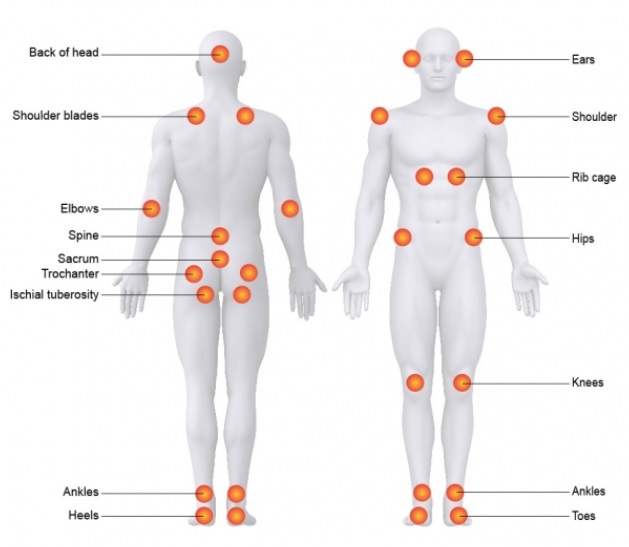
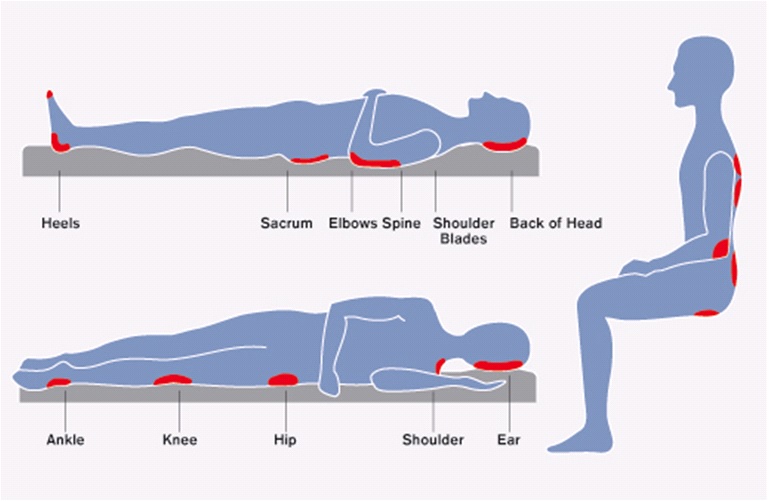
Pressure ulcers most commonly occur over the bony prominences that support the body during lying, standing and sitting. Typical examples of bony prominences commonly at risk of pressure ulcers are:
On the back: The tips of the scapula, elbows, sacrum, heels, back of head
On the front: Knees, iliac crest (hip bones), tops of toes, knees, ears, cheeks
On the side: Ankles, knees, trochanter, ribs, shoulders, ears
Importance of Complete Removal of Pressure
A number of studies have looked at the effect of pressure load on blood supply and the effects on tissue perfusion and damage. The key study below provides evidence and highlights the need for complete pressure elimination.
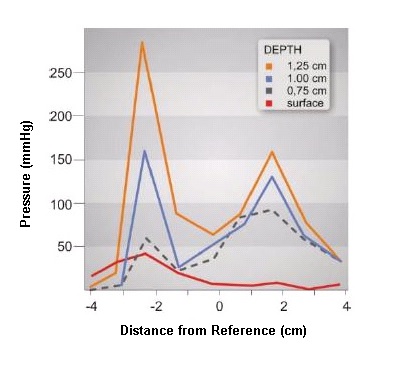
An In-depth Look at Pressure Sores Using Monolithic Silicon Pressure Sensors (Le KM)
Le compared pressures at the tissue interface/surface compared to pressure distribution at different depths into the tissue underlying the trochanter and sacrum.“Pressure is three to five times higher internally near a bony prominence than it is at the skin over the prominence.”“An important inference from this result is that the prevention of pressure sores must entail the removal of the load from the weight bearing bony prominence.”
Total Pressure Relief
A number of studies have looked at the effect of pressure load on blood supply and the effects on tissue perfusion and damage. The key study below provides evidence and highlights the need for complete pressure elimination.
Etiology of Pressure Ulcers (Kosiak, M)
The need for total relief of pressure has long been recognised. Over 40 years ago, Kosiak concluded from his experiments on the effect of sustained and dynamic pressures upon the initiation of pressure damage in muscle tissues that “since it is impossible to completely eliminate all pressure for a long period of time, it becomes imperative that the pressure be completely eliminated at frequent intervals in order to allow circulation to the ischaemic tissues”.
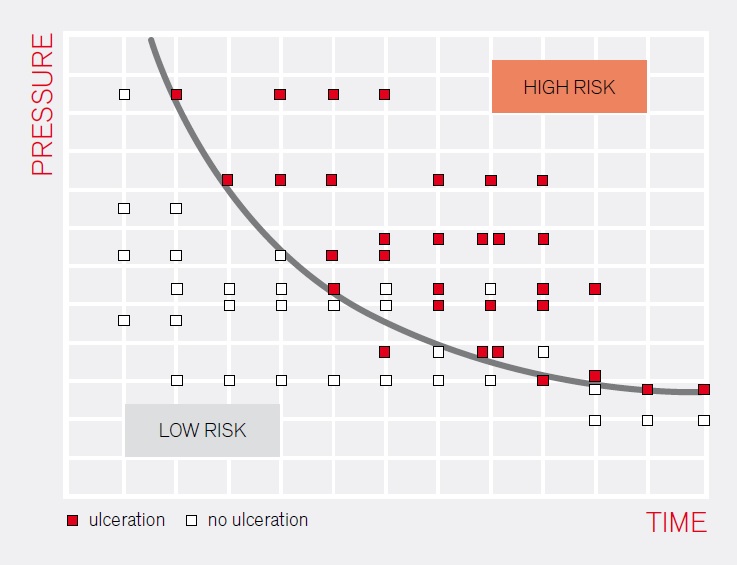
Kosiak also showed the link between pressure and time in the constant pressure group.
“The application of alternating pressures, whereby the tissue was completely free of pressure for five minute intervals, showed consistently less change or no change when compared with tissue subjected to an equivalent amount of constant pressure. This was true even at pressures as high as 240 mm Hg for 3 hours…”
The graph demonstrates the greater the pressure applied the more frequently the pressure should be relieved to prevent tissue damage. (Red squares – damage occurred, Empty squares – damage free).
Capillary Occlusion Pressure
A number of studies have looked at the effect of pressure load on blood supply and the effects on tissue perfusion and damage. The key study below provides evidence and highlights the need for complete pressure elimination.
Micro-injection Studies of Capillary Blood Pressure in Human Skin. Heart (Landis, EM)
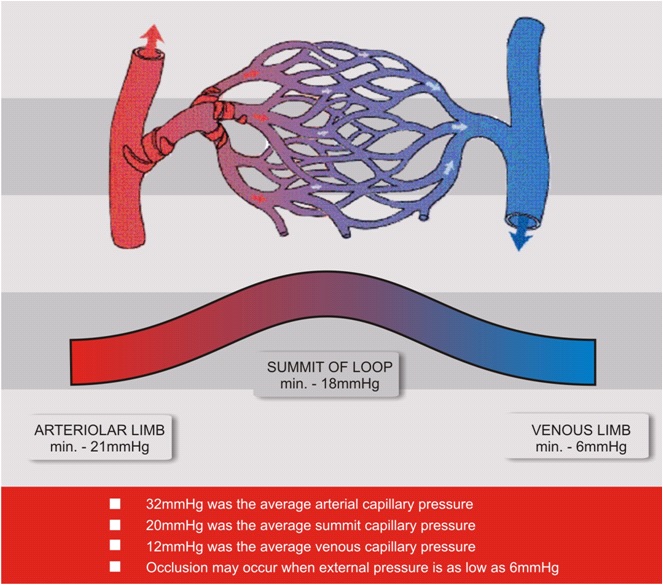
Landis in the late 1920’s among volunteers, and replicated by Williams in 1988 showed the range of capillary pressures that could be measured following various challenges to the peripheral circulation. His work was clear that there was no single constant capillary pressure given that heat, cold and other challenges would markedly change the pressure within the capillaries.
Pressures as low as 6mmHg stopped blood flow, therefore pressures would be likely to reduce if his experiment was to be repeated using elderly ill volunteers.